Debunking Disinformation: The Telegraph Sows Misunderstood Science Amidst Deadly Winter Viral Wave
—Dr. Allen Haddrell teamed up with MaskTogetherAmerica
By Julie Lam
Influenza (flu), respiratory syncytial virus (RSV), and COVID-19 are contributing to a significant number of illnesses, hospitalizations, and deaths this season (2025-2026) in the U.S. and globally, with a notably severe flu season. Instead of supporting public health organizations to promote prevention and infection control, The Telegraph reporter Mattha Busby cooked up right-wing propaganda to stigmatize usage of high filtration masks that experts recommend as a preventive measure. Busby mocked MaskTogetherAmerica’s diverse community of advocates – dominated by people with medical conditions and disabilities, and their allies, calling them ‘zero COVID zealots.’
“The Telegraph article is a poorly written hit piece that misrepresents science to attack a marginalized group. It’s disgusting,” Dr. Allen Haddrell told Julie Lam, founder of MaskTogetherAmerica, who is immunodeficient. Dr. Haddrell is an aerosol scientist who studies aerosol toxicity and pharmacology at University of Bristol. Busby, the journalist who wrote the article, interviewed Julie Lam and added Lam’s masked image to a collage, the article’s main visual, but didn’t include her story—likely because her years of struggles with Long COVID would have contradicted Busby’s penchant for ridicule. People who independently protect their health and work to reduce their own exposure to viral infection should not be subject to mockery. Despite her chronic illness, Lam masked up and travelled from New York City to Bristol to interview Dr. Haddrell in order to write a rebuttal of Busby’s misusing science in such an unproductive fashion. Science being misrepresented or weaponized by Busby shows most obviously, and tragically, his minimization of SARS-CoV-2, the virus that has taken over 7 million lives worldwide.
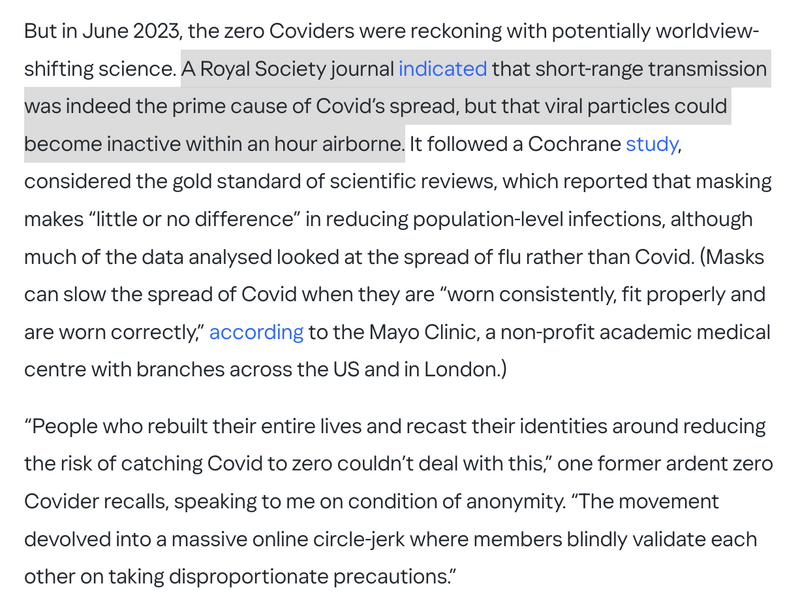
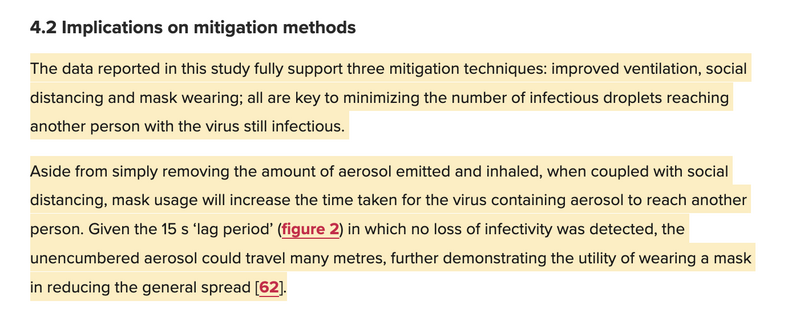
Focusing clearly on science pays off and provides preventive information that should not be discounted or diminished. In 2023, Dr. Haddrell published a laboratory study on viral decay rates of early COVID variants, which suggested that 95% of SARS-CoV-2 gets inactivated in an hour. Busby, without consulting the researcher, misreported: “A Royal Society journal indicated that short-range transmission was indeed the prime cause of COVID’s spread, but that viral particles could become inactive within an hour airborne.” Dr. Haddrell, who wears masks and takes precautions seriously, especially since he works in a BSL-3 Lab, was outraged by the misinterpretation of his research findings, and argued that an hour is a long time for deadly COVID-19 to be airborne! In other words, an airborne virus is living for a long time and sowing a lot of infections in an hour.
In the U.S., CDC researchers estimated that Omicron variants killed 101,300 people between 2022 and 2023 and 100,800 people between 2023 and 2024, based on undercounted data. Dr. Haddrell’s lab studies also showed that Omicron is 1.7 times more aerostable than the Delta variant. Haddrell’s follow-up study, published in 2024, revealed that poor ventilation (≥ 800ppm in CO2 level) helps viruses remain infectious for much longer, which explains why superspreading happens in a crowded room. To consider one well-publicized example, at the Gridiron Dinner in 2022, during the first Omicron wave, 72 out of the hundreds of fully vaccinated guests tested positive.
“Because the Telegraph article is so poorly written, it is unclear exactly what the author is getting at when it comes to our research (the Royal Society article). It claimed that our research showed that the virus is 100% inactivated in the air in about an hour. We did not report that. No one has reported that. They say that we showed that “short-range transmission was indeed the prime cause of COVID’s spread.” We did not show that, because we did not measure transmission. We measured how long the virus was viable in the air. People can use the data we provide to interpret disease transmission studies, but that is something else entirely.” Perhaps Busby’s error relates to an inability to understand the scientific difference between viability and transmission, but writers and reporters do have a responsibility to demonstrate competence as they report. Furthermore, a foundational principle of ethical journalism is that a reporter must fact-check their work thoroughly. Verifying information, especially on a lifesaving mitigation tool, before publication, can avoid irreparable damage far beyond losing readers’ trust – it can also prevent individuals losing their health, or worse, their lives.
Busby’s “worldview-shifting science” against masking also included the controversial Cochrane mask study. The Cochrane study suggests that the analysis of some randomised controlled trials (RCTs) “sort-of suggests” that using surgical masks makes little or no difference, compared to braving crowds with faces uncovered. However, researchers have specified that the quality of the individual studies varied greatly, with high risk of bias, different study designs, and the fact that “adherence with interventions was low in many studies.” The review assessed policy measures to promote mask-wearing rather than the effectiveness of consistent mask-wearing at an individual level. Many of the research studies focused on seasonal flu data, which is less relevant to a year-round airborne virus like SARS-CoV-2 (COVID-19). On the claim that N95 respirators are probably no different than surgical masks, they also clarified that “evidence is limited by imprecision and heterogeneity for these subjective outcomes.” The study concluded that the evidence from the analysed trials was "inconclusive" as to whether promoting mask-wearing interventions helped slow the spread of respiratory viruses.
“Coupling our work to the controversial Cochrane mask study implies that the two are reporting that masks are ineffective. This is simply not true. In our article, we make it clear that masking is indeed incredibly important for mitigating spread. We also make it explicitly clear that even though the decay rates are slightly faster than originally reported, the virus remains viable in the air for a long enough time.” Dr. Haddrell points to a section in the article that Busby cites.
The Royal Society article actually promotes mask usage! In Dr. Haddrell’s lab, it is mandatory to wear a mask. Researchers also wear other personal protective equipment, including latex gloves (doubled, as in two gloves for each hand), and lab coats.
“To work in a high containment lab, safety is paramount. Airborne transmission from the experiment is minimized by the use of both the flexible film isolator and the design of the CELEBS (Controlled Electrodynamic Levitation and Extraction of Bioaerosol onto a Substrate) instrument. Thus, the greatest risk in our work would come from the handling of the sample, followed by inadvertently/accidentally touching one’s face. The masks protect from that. In general, BSL-3 labs require masking because the users are surrounded by a high concentration of a transmissible disease. In such an environment, masking is critical as they dramatically lower any and all exposure.”
In addition to masking, Dr. Haddrell also keeps the air quality of his high containment lab at a high standard.
“The air in the aerobiology lab is exchanged at a tremendous rate. It’s typically around 10 -12 ACH (Air Changes per Hour), but can be as high as 20. Fresh air brought into the lab is HEPA-filtered. Collectively, this means that the air in the lab is extraordinarily clean.” Dr. Haddrell also added that experiments are undertaken within a levitation chamber, which itself is placed in a large plastic bag with sleeves (see photo). This physically protects the user from the virus sample— a unique safety feature of their lab.
Fair and impartial reporting is a foundational principle of journalistic ethics. Busby should have verified information from multiple sources and provided context instead of deliberately distorting the facts of science and the facts of people’s stories. Busby simply reveals an unfounded personal hatred against virus mitigation.
Busby chose to attack people who wore masks that appeared to be young and physically healthy from the outside, and he excluded examples of elderly people and disabled people he had interviewed. Having learned through interviewing thousands of Long COVID patients, researchers, and medical professionals for a pandemic documentary project, Julie explained to Busby that everyone is only an infection away from becoming chronically ill or disabled.
A news organization discriminating against a minority group dominated by immunocompromised and disabled people— is shameful ableism taken to new heights. The Telegraph is notorious for publishing anti-mask rhetoric.[a] [b] However, on July 24 2020, during the first deadly wave of the pandemic, The Telegraph published a pro-mask article by Jennifer Rigby. Rigby interviewed historians to compare temporal changes on the backlash against masking. Rigby’s research included a dark historical reference that contradicts inflexible mask resistance for die-hard individual liberty— a French doctor died from refusing to mask. In the story, the masked Chinese doctor lived.
During the interview, Busby told Julie that he never wore a mask, and he revealed his mission to use his power to intimidate mask advocates one by one. His methodology: grabbing, amassing posts from social media platforms of public figures/influencers and MaskTogetherAmerica— then branding those who put their health and community first as ‘Left-wing” and as people, who by his account, are living in fear.
Busby quotes Taylor Lorenz saying “If ur [sic] not masking ur absolutely facilitating eugenics” —to begin a section featuring celebrities joining our collective movement to end pandemic denialism. To Busby, even promoting infection control is ridiculous. Though pandemic denialism is clearly horrible, Busby is using his power to protect it. Should we call him the ‘Million COVID Zealot’?
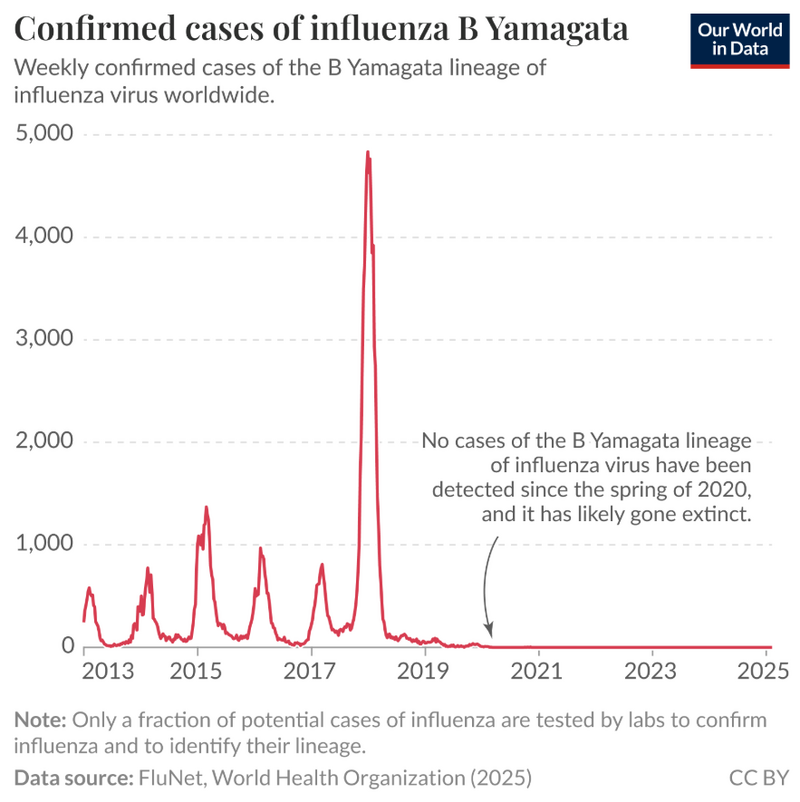
All jokes aside, many studies have shown that wearing a mask, especially a well-fitted N95 mask [1][2][3][4][5][6], combined with HEPA filtration [7][8][9] provides valuable protection against COVID-19. ( See our research here.) Universal masking and other public health interventions during the early days of the COVID-19 pandemic likely eliminated the influenza B/Yamagata lineage. No confirmed cases of this strain have been reported worldwide since March 2020. Collective action can beat deadly viruses. Misinformation fuels infection!
Dr. Haddrell said that airborne transmission of disease is not inevitable. “It’s something we can control. We know this from what happened with influenza B Yamagata; it disappeared due to the COVID restrictions. This is not to advocate for these restrictions all the time, but rather to identify that it is possible. We have learned a lot during the pandemic, and we have so many tools in our toolkit now that we could be using to limit airborne disease transmission. We just need to use them. Any of them.”
Julie Lam caught COVID-19 close to the end of 2021. Despite being up-to-date with vaccination, she couldn’t recover. After seeing over 30 specialists, 3 years later, she was diagnosed with Long COVID due to organ damage, sleep apnea, immune dysregulation, dysautonomia, microclots, mitochondrial dysfunction, metabolic dysfunction, and reactivation of Herpes Zoster virus a.k.a. Shingles. Dr. Haddrell caught COVID-19 in 2022. Though he doesn’t have Long COVID, he said having COVID was terrible. “Long COVID is a terrible and still poorly understood condition that affects millions. It’s the elephant in the room that no one wants to talk about, and it’s costing society a lot in terms of both healthcare costs and quality of life. The fact that it is avoidable through thoughtful mitigation strategies makes it even more tragic.”